Exercise’s Impact on Cognition
It’s not news that the brain changes with age. Significant changes in regions of the brain occur in healthy adults as they age, based on MRI studies.(1) The caudate, cerebellum, hippocampus, and association cortices shrunk substantially. This shrinkage in the hippocampus and the cerebellum accelerates with age. The hippocampus, the site for new memory formation, is involved with learning and emotion with a rich supply of estrogen and progesterone receptors. The cerebellum coordinates voluntary movements including all conscious muscular activity, balance, coordination, and speech.
Incidence of Dementia
The United States is experiencing both a declining birth rate and an increased average life span. This combination will increase the percentage of people over the age of 65 to 19.6%, resulting in a total of 71 million people by the year 2030.(2) The number of people over the age of 80 is also expected to increase to 19.5 million by 2030.(2) These changes will greatly increase the number of people with dementia since 6% to 10% of North American individuals aged 65 or older have dementia; this increases to 30% in those aged 85 or over.(3)
Dementia, or senility, is a difficult-to-define cluster of symptoms that include memory loss, loss of vocabulary, and loss of motor function in the absence of a change in the level of consciousness. Dementia can be measured qualitatively by verbal memory tests such as the Blessed Orientation-Memory-Concentration test, comprising six questions as listed in the following table:
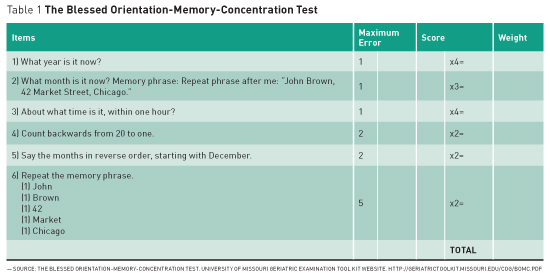
The scores from each of the table’s six items are multiplied to produce a weighted score. Score 1 for each incorrect response; weighted error scores greater than 10 are consistent with dementia.(4)
Exercise Affects the Brain
The incidence of Alzheimer’s dementia can be used as a measurement of brain health.(5) As part of his study “Exercise Is Associated With Reduced Risk for Incident Dementia Among Persons 65 Years of Age and Older,” Eric B. Larson, MD, MPH, et al asked 1,740 mentally healthy men and women over the age of 65 how many days per week over the past year they had exercised for at least 15 minutes. The incidence of Alzheimer’s disease (AD) was significantly higher for individuals who exercised fewer than three times per week (19.7 per 1,000 person-years) compared with those who exercised more than three times per week (13 per 1,000 person-years). These results were not influenced by the E4 alleles on the apolipoprotein gene, which indicates a genetic predisposition for AD.
Laura Podewils et al studied the relationship between physical activity and dementia in 3,375 men and women over the course of 5.4 years.(6) Physical activity in these individuals over the age of 65 was assessed via the Minnesota Leisure Time Questionnaire. The subjects were questioned regarding the frequency and duration of their physical activity over the previous two weeks. Like Larson et al, this study found that increased exercise decreased the incidence of Alzheimer’s dementia.
The Mini-Mental State Exam can be used as a measure of cognitive ability or impairment. The 30-point questionnaire commonly used by health care providers screens for dementia, evaluates cognitive impairment, and follows cognitive change over time, making it an effective way to document an individual’s response to treatment.(7) Kristine Yaffe, MD, et al used the Mini-Mental State Exam to show that cognitive performance increases as the number of blocks walked per week increases.(8) The study involved 5,925 women over the age of 65 over a six- to eight-year period.
The most objective measure of cardiovascular fitness is the measurement of the maximum rate of oxygen consumption as measured during incremental exercise—milliliters of oxygen per kilogram of body mass per minute. A subjective measure of exercise amount or duration is not as accurate as the above direct measure, which is called maximum oxygen consumption or VO2 max. Deborah Barnes, PhD, et al conducted a six-year study of 349 individuals over the age of 55 measuring both VO2 max and subjective measures of fitness. Barnes found only the lower levels of VO2 max correlated with cognitive decline.(9) The four studies mentioned show a positive cognitive benefit from exercise. A meta-analysis performed by Colcombe and Kramer from 1966 to 2001 examined 18 studies of fitness training and cognitive function in nondemented older adults. They concluded that fitness training had a positive influence on cognition.(10)

Prospective controlled human studies provide more robust data than both animal and uncontrolled studies. Stanley J. Colcombe et al were the first to show in a prospective controlled setting that increases in cardiovascular fitness in humans results in increased functioning of the prefrontal and parietal cortices. These data suggest that increased cardiovascular fitness can affect improvements in the plasticity of the aging human brain and may serve to reduce both biological and cognitive senescence in humans.(11) In addition, women tended to exhibit the greater benefit.(12) In a literature review, Kramer et al complemented these data through the use of MRI, which is very accurate in the brain. Through this technique, Kramer and colleagues concluded that older adults who participated in the aerobic training group demonstrated a significant increase in gray matter volume in regions of the frontal and superior temporal lobe when compared with controls. The results suggest that even relatively short exercise interventions can begin to restore some of the losses in brain volume associated with normal aging.(12)
Animal studies offer some insight into how aerobic exercise benefits brain function. Aerobic exercise increases brain function in both young and old animals. Aerobic exercise increases the levels of brain-derived neurogenic factor (BDNF) and insulinlike growth factor 1 (IGF-1). BDNF has been shown to regulate neurotransmitters, including dopaminergic and cholinergic systems and may be playing an important role in the exercise-induced effects on the brain.(13) BDNF may be involved in the postexercise changes seen on a brain MRI. In addition, IGF-1 may be mediating the effects of exercise on BDNF, neurogenesis, and cognitive performance. Animal studies provide information on the effects of exercise that is difficult to obtain in human intervention studies. The sum of these animal studies overlaps with results from human studies and suggests that exercise is an effective enhancer of neurocognitive functioning in both young and old animals.(12)
AD, the most common form of dementia, shares many age-related pathophysiological features of type 2 diabetes, including insulin resistance, disrupted glucose metabolism in nonneural tissues, peripheral oxidative and inflammatory stress, amyloid aggregation, neural atrophy, and cognitive decline. Brain insulin resistance appears to be an early and common feature of AD, a phenomenon accompanied by IGF-1 resistance, promoting cognitive decline independent of classic AD pathology.(14) Such a large set of shared features suggests shared etiologies.
Recommendation
High-intensity interval training (HIIT) is a type of endurance training involving short periods of maximal effort followed by periods of maintenance or recovery effort. What can differ is the timing and type of endurance exercise. A typical cycling HIIT pattern may be four to six maximal 30-second cycling sprints separated by 4.5-minute recovery periods of comfortable cycling. When HIIT is compared with longer steady endurance training, the HIIT patterns show increased mitochondrial density in muscle cells and greater muscle performance improvements.(15,16)

Get a Free Subscription to Today’s Geriatric Medicine
This article was featured in Today’s Geriatric Medicine.
Today’s Geriatric Medicine is a bimonthly trade publication offering news and insights for professionals in elder care.
Get a Free Subscription to Today’s Geriatric Medicine
This article was featured in the Jan/Feb 2016 issue of Today’s Geriatric Medicine (Vol. 9 No. 1 P. 26). Written by Robert Drapkin, MD
Robert Drapkin, MD, a medical oncologist and competitive bodybuilder in Clearwater, Florida, specializes in helping elderly adults achieve a healthful lifestyle to combat illnesses or disease and to extend lifespan.
References
1. Raz N, Lindenberger U, Rodrigue KM, et al. Regional brain changes in aging healthy adults: general trends, individual differences and modifiers. Cereb Cortex. 2005;15(11):1676-1689.
2. Chapman DP, Williams SM, Strine TW, Anda RF, Moore MJ. Dementia and its implications for public health. Prev Chronic Dis. 2006;3(2):A34.
3. Hendrie HC. Epidemiology of dementia and Alzheimer’s disease. Am J Geriatr Psychiatry. 1998;6(2 Suppl 1):S3-S18.
4. The Blessed Orientation-Memory-Concentration Test. University of Missouri Geriatric Examination Tool Kit website. http://geriatrictoolkit.missouri.edu/cog/bomc.pdf.
5. Larson EB, Wang L, Bowen JD, et al. Exercise is associated with reduced risk for incident dementia among persons 65 years of age and older. Ann Intern Med. 2006;144(2):73-81.
6. Podewils LJ, Guallar E, Kuller LH, et al. Physical activity, APOE genotype, and dementia risk: findings from the Cardiovascular Health Cognition Study. Am J Epidemiol. 2005;161(7):639-651.
7. Pangman VC, Sloan J, Guse L. An examination of psychometric properties of the mini-mental state examination and the standardized mini-mental state examination: implications for clinical practice. Appl Nurs Res. 2000;13(4):209-213.
8. Yaffe K, Barnes D, Nevitt M, Lui LY, Covinsky K. A prospective study of physical activity and cognitive decline in elderly women: women who walk. Arch Intern Med. 2001;161(14):1703-1708.
9. Barnes DE, Yaffe K, Satariano WA, Tager IB. A longitudinal study of cardiorespiratory fitness and cognitive function in healthy older adults. J Am Geriatr Soc. 2003;51(4):459-465.
10. Colcombe S, Kramer AF. Fitness effects on the cognitive function of older adults: a meta-analytic study. Psychol Sci. 2003;14(2):125-130.
11. Colcombe SJ, Kramer AF, Erickson KI, et al. Cardiovascular fitness, cortical plasticity, and aging. Proc Natl Acad Sci U S A. 2004;101(9):3316-3321.
12. Kramer AF, Erickson KI, Colcombe SJ. Exercise, cognition, and the aging brain. J Appl Physiol (1985). 2006;101(4):1237-1242.
13. Knüsel B, Winslow JW, Rosenthal A, et al. Promotion of central cholinergic and dopaminergic neuron differentiation by brain-derived neurotrophic factor but not neurotrophin 3. Proc Natl Acad Sci U S A. 1991;88(3):961-965.
14. Talbot K, Wang HY, Kazi H, et al. Demonstrated brain insulin resistance in Alzheimer’s disease patients is associated with IGF-1 resistance, IRS-1 dysregulation, and cognitive decline. J Clin Invest. 2012;122(4):1316-1338.
15. Gibala M. Molecular responses to high-intensity interval exercise. Appl Physiol Nutr Metab. 2009;34(3):428-432.
16. Billat VL. Interval training for performance: a scientific and empirical practice. Special recommendations for middle- and long-distance running. Part I: anaerobic interval training. Sports Med. 2001;31(1):13-31.



 Evidence in Favor: Cognitive Benefits in Dementia
Evidence in Favor: Cognitive Benefits in Dementia
 “People with diabetes are living longer now, which is incredibly exciting,” says Rita Kalyani, MD, MHS, an associate professor of medicine in the division of endocrinology, diabetes, and metabolism at Johns Hopkins School of Medicine. But “it’s important to recognize [the potential for accelerated muscle loss] because it can significantly impact quality of life for people with diabetes and also mortality.”
“People with diabetes are living longer now, which is incredibly exciting,” says Rita Kalyani, MD, MHS, an associate professor of medicine in the division of endocrinology, diabetes, and metabolism at Johns Hopkins School of Medicine. But “it’s important to recognize [the potential for accelerated muscle loss] because it can significantly impact quality of life for people with diabetes and also mortality.” The presence of insulin resistance, which is the key feature of type 2 diabetes, appears to be a major pathway. “Insulin resistance is associated with decreased protein synthesis in the muscle,” Kalyani says. One of the key roles of insulin is to drive nutrients (ie, glucose) from the blood into skeletal muscle tissue and stimulate protein synthesis. In type 2 diabetes, however, insulin signaling is impaired; insulin is not able to effectively drive glucose into the muscle tissue, and the muscle cannot synthesize new protein rapidly enough to keep pace with natural muscle degradation.(13)
The presence of insulin resistance, which is the key feature of type 2 diabetes, appears to be a major pathway. “Insulin resistance is associated with decreased protein synthesis in the muscle,” Kalyani says. One of the key roles of insulin is to drive nutrients (ie, glucose) from the blood into skeletal muscle tissue and stimulate protein synthesis. In type 2 diabetes, however, insulin signaling is impaired; insulin is not able to effectively drive glucose into the muscle tissue, and the muscle cannot synthesize new protein rapidly enough to keep pace with natural muscle degradation.(13)