Useful Tips for Relieving Back Pain During Pregnancy
While there is no doubt that pregnancy and motherhood are the happiest moments in a woman’s life, however, it comes with its own share of problems and challenges.

While there is no doubt that pregnancy and motherhood are the happiest moments in a woman’s life, however, it comes with its own share of problems and challenges.
On January 18th, 2017 Rudy Gay, forward for the Sacramento Kings, drove the baseline against the Pacers and crumbled to the floor without being touched. He didn’t get up and was carried off the court. Gay had torn his Achilles tendon, a devastating injury for a pro, and really bad news for any athlete.

When you have a serious injury, such as breaking your arm, tearing your ACL ligament or even one as simple as banging your knee against a hard object, the limitations of functional capacity that these injuries have on your body can be quite debilitating
Water babies, that’s us. We’re at home in liquid from pre-birth and we seem to naturally gravitate to it. We love the ocean, the lake the pool, the hot tub, and the bathtub. What is it about water that means so much to us? It surrounds us, it cradles us, and it supports us. We’re nearly weightless in water.

Kinesiotherapy (KT) is a highly specialized and yet extremely adaptable therapeutic discipline. A Registered Kinesiotherapist (RKT) is equipped with knowledge and skills to bridge any gap between acute illness and physical wellness. The RKT uses two fundamental modalities, exercise and education, to help improve functional loss in their clients.

The foot is where movement begins requiring mobility to initiate daily and sport specific movements. However, the knee however, requires stability with daily movements, but more importantly, dynamic sport movements such as soccer or football. The hip, like the ankle, requires mobility, to perform such simple movements as sit to stand, climbing stairs and other functional movements. In this article, we will review the anatomy of the hip, common injuries to the hip, functional assessments and training strategies to work with clients with previous injuries.

Hip joint with supporting ligaments
Let’s look at the basic anatomy of the hip. The hip joint is a multi-axial ball and socket joint between the femoral head and the acetabulum, similarly to the shoulder joint. The hip is surrounded in white, several ligaments that provide support and stability.
The labrum attaches to the acetabulum deep within the socket between the femur and acetabulum. The joint is covered by a capsule blended with three strong ligaments: iliofemoral or “Y” ligament, which resists extension, the ischiofemoral ligament, which resists extension and internal rotation, and the pubofemoral ligament, which resists abduction.
Muscularly, the glute medius and minimus are located along the anterolateral aspect of the hip to stabilize in the frontal pane, whereas the glute maximus, is located in the sagittal plane posteriorly to facilitate hip extension.
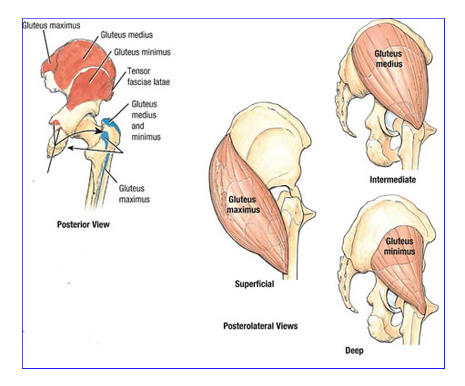
Supporting muscles around the hip
There are different types of injuries the hip can sustain. The most common are the hip osteoarthritis, iliotibial band syndrome and total hip replacement. In this next section, we will review each condition providing a deeper understanding of each.
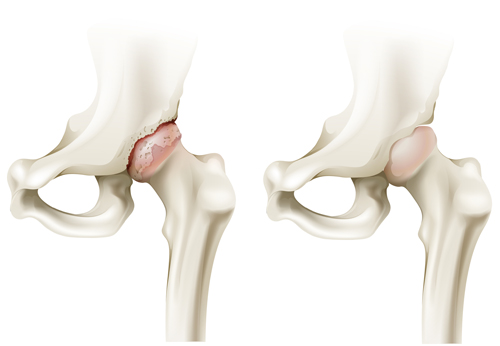
Osteoarthritic hip on left, normal hip on right
a. Hip osteoarthritis(OA)
Mechanism of injury/pathophysiology: A degenerative process of varied etiology which includes mechanical changes within the joint. O.A. affects some 40% of those aged over 65 in the community may have symptomatic OA of the knee or hip(Zhang, W. et al 2007).
Pathophysiology: Osteoarthritis (OA) is a relatively common musculoskeletal disorder, with a high prevalence that increases with age. O.A. is a degenerative process of varied etiology, which includes mechanical changes within the joint (Pisters, M., et al 2007).
Risk Factors: Excessive weight born on hip joint, muscle imbalance, repetitive stressors.
Sign and symptoms: Pain in the a.m. described as “achy” that decreases as the day progresses, pain with weight bearing or walking, difficulty squatting, and lateral thigh discomfort. Patients will describe of pain and stiffness in the a.m. described as “achy.” During the day, movement and activity, improves mobility and activity(Fernandes, L et al 2010). However, the volume of activity if too much, will increase pain. Patients typically have pain with weight bearing or prolonged walking, difficulty squatting, and lateral thigh discomfort.
Medical treatment: Non steroidal (NSAIDS)(examples are Ibuprofen/Advil).
Iliotibial band syndrome
b. Iliotibial band syndrome(ITB)
Mechanism of injury: Iliotibial band syndrome (ITBS) is a common injury of the lateral(outside) aspect of the knee particularly in runners, cyclists and endurance sports. ITBS is the most common running injury(Ellis, R et al 2007).
Pathophysiology: ITB syndrome is a non-traumatic overuse injury caused by repetitive friction/rubbing of the distal(farthest) portion of the iliotibial band (ITB) over the lateral femoral epicondyle with repeated flexion and extension of the knee.
Contributing/Risk Factors:
• Muscle imbalances/weakness: per the research and my clinical experience, hip flexors and quadriceps are stronger and than the hamstrings.
• Shoe support-important to rotate running shoes every 6 months or 500 miles according to multiple podiatrists I have worked with over the years.
• Increased bouts of running, altered foot mechanics-ie. Orthotics or need for orthotics.
• Lack of stretching, particularly tight ITB, hip flexors and quadriceps. Contributes to increasing compression along the outer hip.
Sign and symptoms: Lateral knee pain over the lateral condyle of the femur described as “dull/achy” that gradually develops & worsens particularly with running. Pain then becomes “sharp” in nature.
c. Total hip replacement
Mechanism of injury: Osteoarthritis is a musculoskeletal condition that develops over time affecting primarily the hip and knee joints. O.A. affects some 40% of those aged over 65 in the community may have symptomatic OA of the knee or hip(Zhang, W. et al 2007).
Pathophysiology: Osteoarthritis (OA) is a relatively common musculoskeletal disorder, with a high prevalence that increases with age. O.A. is a degenerative process of varied etiology, which includes mechanical changes within the joint (Pisters, M., et al 2007). Significant pain, decreased mobility and compromised function, are the primary reasons, a person would typically undergo a total joint arthoplasty(joint replacement). Total joint arthroplasty is a highly efficacious and cost-effective procedure for moderate to severe arthritis in the hip(Santaguida, P. et al 2008).
A simple functional test to assess a client’s movement pattern, is the squat. The squat is a classic fundamental primal movement that someone typically performs almost on a daily basis. With this test, you can observe how the client’s ankle, knee, hip and back moves compared to normal movement patterns.
What am I looking for?
The approach to assessment is all about asking and answering questions about movement:
• How does the client start, finish the movement?
• What strategies do they use? Do they have the appropriate flexibility to perform the movement?
• Is stability a problem? Are there compensations elsewhere in the movement sequence?
How do I interpret the movement?
• It is important to observe the client in both the frontal and sagittal planes
• Observing globally first, then examine how the entire kinematic chain is working as it relates to timing and sequence to achieve the movement
1. Functional squat
The squat is a classic fundamental primal movement that someone typically performs almost on a daily basis. Whether it is to perform to pick something up or move an item. Therefore, it is important to assess the movement pattern a client uses during this movement.

Squat in frontal view; Squat in side view
What is required in a squat?
• Adequate ankle mobility, knee stability, hip mobility, lumbar spine(lumbo-pelvic junction) stability

In place lunge
Observations:
• Note the overall quality and range of movement in the frontal plane and sagittal plane
• Note the symmetry or lack of symmetry with the movement
• Note the point of transition from descending to ascending
• Note if there is an shaking(juttering), which indicates weakness in the lumbo-pelvic junction affecting the entire kinematic chain
Another simple assessment is an in place lunge, which examines one’s control through the entire kinematic chain. The lunge is another fundamental primal movement. The lunge is a dynamic movement that is typically performed during daily activities (stooping down to pick something up) or as part of an athletic movement. This test examines ankle control, knee control and pelvic movement in the sagittal plane.
With any injury, the most important thing to remember is the type of injury, healing time and prior level of function of the client. Let’s begin with ankle sprains.

SLS stance with TRX
a. Hip Osteoarthritis(O.A.)

ITB stretch
Recommendations for training: Aqua therapy has been shown in the research to significantly reduce pain, improved physical function, strength, and quality of life(Hinman, Rana S., et al 2007), stretching ITB, hip flexors, quadriceps and hamstrings, strengthening weaker hip abductors(glute medius/minimus). Strengthening specifically hip abductors in various studies when compared to general strengthening, resulted in significant reduction in knee pain, objective change in functional outcome tests, physical function and daily activities(Bennell, K.L., et al. 2010 & Hernández-Molina, G et al. 2008). Core strengthening should also be an integral part of the training program.
b. ITB Syndrome
Recommendations for training: Important to keep stretching the ITB after exercise. Client education on the changing of running shoes every 500 miles or 6 months is key. Resistance training should focus on strengthening weaker phasic muscles (glute medius, minimus and maximus), which are required to stabilize and push off during running. Dynamic core strengthening should always play an integral role of training. Use of aqua therapy can be extremely beneficial and relaxing. It is very important to educate the client on the importance of cross training(ie. yoga, pilates, hiking, and swimming to condition the lower extremity muscles.
c. Hip replacement(THR)

Bridging with physioball
Recommendations for training: Prior to commencing training, it is important to clarify with client, that there are no other underlying health issues. Important to follow hip precautions: avoidance of crossing affected leg towards midline(adduction), and squatting past hip flexion 90 degrees. Training should focus on strengthening weak glute medius/minimus, glute maximus and hamstrings. Effective and safe exercises include; in place lunges, diagonal lunges, seated leg extension and seated leg curl machine. Core strengthening should also always begin with static exercises, and then progressed to dynamic accordingly. Safe and effective core strengthening exercises include; standing trunk rotation with tubing or cable, four point planks, and side planks. Safe dynamic core strengthening exercises include bridging with physioball, single leg bridge with physioball, traveling forward lunge with medicine ball trunk rotation, and four-point plank on physioball as examples.
The hip is a complex unit thitbdat is comprised of a multitude of ligaments, tendons, connective tissue, muscles that synergistically initiate and correct movement, and stabilize when an unstable environment. Understanding the anatomy, biomechanics and weak links of the hip, common injuries and evidenced based training strategies, should provide you with the insight to better understand and work with clients with these kind of injuries more confidently.
Written by Chris Gellert, PT, MMusc & Sportsphysio, MPT, CSCS, AMS.
Chris is the CEO of Pinnacle Training & Consulting Systems (PTCS). A continuing education company, that provides educational material in the forms of home study courses, live seminars, DVDs, webinars, articles and min books teaching in-depth, the foundation science, functional assessments and practical application behind Human Movement, that is evidenced based. Chris is both a dynamic physical therapist with 14 years experience, and a personal trainer with 17 years experience, with advanced training, has created over 10 courses, is an experienced international fitness presenter, writes for various websites and international publications, consults and teaches seminars on human movement.
REFERENCES
Bennell, K.L., et al. 2010, ‘Hip strengthening reduces symptoms but not knee load in people with medial knee osteoarthritis and varus malalignment: a randomized controlled trial,’ Osteoarthritis and Cartilage, vol. 18, issue 5, pp. 621–628.
Ellis, R., et al., 2007, ‘Iliotibial band friction syndrome—A systematic review,’ Manual Therapy, vol. 12, pp. 200–208.
Fernandes, L., et al 2010, ‘Efficacy of patient education and supervised exercise vs. patient education alone in patients with hip osteoarthritis: a single blind randomized clinical trial,’ Osteoarthritis and Cartilage, vol. 18, issue 10, pp. 1237–1243.
Goodman, Catherine., Boissonnault, William., 1998, G. Pathology: Implications for the Physical Therapist, W.B. Saunders Company, Philadelphia, pp. 267-274, 279-292, 318-328, 412- 417, 609-610, 614-615, 617-621, 660-667, 736-745, 748-755.
Hernández-Molina, G et al. 2008 ‘Effect of therapeutic exercise for hip osteoarthritis pain: Results of a meta-analysis,’Arthritis Care & Research, vol. 59, issue 9, pp. 1221-1228.
Hinman, Rana S., et al 2007, ‘ Aquatic Physical Therapy for Hip and Knee Osteoarthritis: Results of a Single-Blind Randomized Controlled Trial,’ Journal of Physical Therapy, vol. 87, no. 1, pp. 32-43.
Pisters, M., et al., 2007, ‘Exercise adherence improving long-term patient outcome in patients with osteoarthritis of the hip and/or knee, Arthritis Care & Research, vol. 62,
Santaguida, P. et al 2008, ‘Patient characteristics affecting the prognosis of total hip and knee joint arthroplasty: a systematic review,’ Canadian Journal of Surgery, vol. 51, issue 6, pp. 428-436.
Zhang, W., et al., ‘OARSI recommendations for the management of hip and knee osteoarthritis, Part I: Critical appraisal of existing treatment guidelines and systematic review of current research evidence,’ Osteoarthritis and Cartilage, vol. 15, issue 9 pp. 981–1000.

The foot is where movement begins, requiring mobility to perform simple functional movements. The knee however, requires stability with daily movements, but more importantly, dynamic sport movements such as soccer or football. In this article, we will review the anatomy of the knee, common injuries of the knee, functional assessments and training strategies to work with clients with previous injuries.
Basic anatomy of the knee
Let’s look at the anatomy of the knee.. The joint is vulnerable when it comes to injury, because of the mechanical demands placed upon it and the reliance for soft tissue to support the knee. There are two primary joints within the knee, the tibiofemoral joint and the patellofemoral joint.
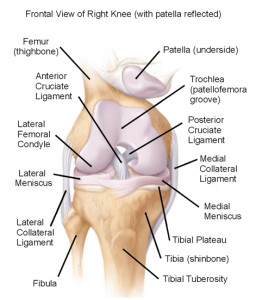
Figure 2. Structures within the knee joint
Knee Joints
a. Tibiofemoral joint: Is a hinge joint that permits some rotation between the distal end of the femur and proximal end of tibia. The joint capsule surrounds the femoral condyles and tibial plateaus and provides stability to the knee by the medial collateral ligament(MCL) and the lateral collateral ligament (LCL).
b. Patellofemoral joint: Is formed by the patella(knee bone) that glides in the trochlear groove of the femur. The height of the lateral femoral condyle helps prevent lateral subluxation, while soft tissue surrounds the joint to increase stability. This is seen in figure 3.
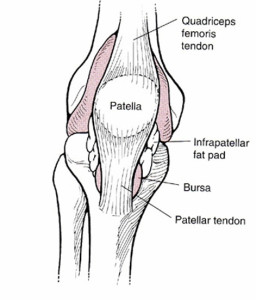
Figure 3. Patellofemoral joint
Primary structures within the knee joint: ligaments and mensici
Several ligaments described below provide stability at the knee joint.
a. Collateral ligaments: The two primary supporting ligaments are the medial collateral ligament (MCL), which is along the inside of the knee. The MCL is a thinner and weaker ligament biomechanically, making it more susceptible to injury more often injured per the research. While the lateral collateral ligament(LCL) is along the outside or lateral aspect of the knee providing lateral knee stability.
b. Anterior cruciate ligament(ACL): is the most commonly injured knee ligament and is taut during knee extension. It originates more proximally on the femoral side than the posterolateral (PL) bundle. It inserts anteromedially(front and to inner side) on the tibia. The ACL limits and controls forward translation of tibia on the femur and limits tibial rotation.
c. Menisci: the menisci are fibro cartilaginous discs located on the articular surface of the tibia along the medial and lateral tibial plateaus. The outer portion of the meniscus(lateral meniscus)is oval shaped (O) and thick. Attaching at the anterior and posterior horns via coronary ligaments.
Vascularity: The middle third and inner third of both menisci are relative avascular. The medial meniscus is more C-shaped, and thinner in structure. Both menisci receive nutrition through synovial diffusion and from blood supply to the horns of the menisci.
Function of the menisci: The menisci provide shock absorption, joint lubrication and stabilization.
There are several common injuries that affect the knee. The most common are patella femoral syndrome(PFS), osteoarthritis(O.A.) and anterior cruciate ligament(ACL) injuries.
In this next section, we will review each condition providing a deeper understanding of each.
a. Patellofemoral syndrome
Pathophysiology/sign and symptoms: PFS is a condition where the patella does not translate biomechanically in the trochlear groove between the femoral condyles. Here the patella is positioned in either a tilt, glide or rotation accompanied by diffuse, achiness in the front of the knee.
Contributing Factors(Evidence Based Research): Several studies have shown that decreased flexibility of quadriceps and hip flexors(Lankhorst et al. 2012 & Meira et al. 2011) contribute to PFS. Decreased hip abductor strength has been shown a significant factor seen in multiple studies as contributing to PFS (Khayambashi, H., et al. 2012, Meira et al, (2011), Bolgla et al. (2008),Cichanowski et al. (2007), and Robinson et al. (2007).
Other factors include prolonged wearing of high heels, muscle imbalances(quadriceps>hamstrings).
b. Osteoarthritis(OA) of the knee

Figure 4. Osteoarthritis of knee
Pathophysiology/sign and symptoms: A degenerative process of varied etiology, which includes mechanical changes within the joint as seen in figure 4.
Risk Factors: Excessive weight born on hip joint, muscle imbalance, repetitive stressors.
Sign and symptoms: Pain in the a.m. described as “achy” that decreases as the day progresses, pain with weight bearing or walking, difficulty squatting, and lateral thigh discomfort.
c. Anterior cruciate ligament injuries
In the last several years, there has been more news about the incidence of ACL injuries. The incidence rate is greatest between the ages of 16 and 18 years. Female athletes are 3-9x more likely to sustain an ACL injury then male athletes. This results in at least 200,000 ACL reconstructions are performed each year in the United States, with estimated direct costs of $3 billion (in U.S. dollars) annually (Frobell, R., et al 2010).
Figure 5. Mechanism of injury for ACL tear
Pathophysiology/Mechanism of Injury: The knee is struck while in hyperextension, forcing tibia anterior(forward)on the femur, as seen in figure 5. The ACL can also be injured with same mechanism of injury with combined with medial rotation of the lower extremity(LE). This creates instability and a direct disconnect the nervous system to the musculoskeletal system because of the “lack of control” within the knee joint.
Common assessments
One great test to assess a client’s movement pattern, is the squat. The squat is a classic fundamental primal movement that someone typically performs almost on a daily basis. With this test, you can observe how the client’s ankle, knee, hip and back moves compared to normal movement patterns. This is seen in the figure below.

Figure 6. Squat in frontal and side view

Figure 7. In place lunge
Another simple assessment is an in place lunge, which examines one’s control through the entire kinematic chain. The lunge is another fundamental primal movement. The lunge is a dynamic movement that is typically performed during daily activities (stooping down to pick something up) or as part of an athletic movement.
This test examines ankle control, knee control and pelvic movement in the sagittal plane. Lastly, a diagonal traveling forward lunge looks at the ability of the client to control ankle, knee, hip, and pelvic movement in both the sagittal and frontal planes. This is not only a functional movement, but very effective for sport specific clients.
Training strategies and programming for knee injuries

Figure 8. Traveling forward lunge
With any injury, the most important thing to remember is the type of injury, healing time and prior level of function of the client.
a. Patellofemoral syndrome
Recommendations for training: Continued stretching of tight hip flexors, ITB, and hamstrings is fundamental. Client should be taught initially static core strengthening exercises, and then progressed to dynamic core strengthening as appropriate. Client would also benefit from education on shoes with respect to type that are most effective for them, and to cross train utilizing, such as hiking, yoga, pilates, and swimming. Lastly, to alter running surfaces(if client runs) and educating the client about changing their shoes every 500 miles or 6 months for maximum stability and control.
b. Osteoarthritis of knee (O.A.)
Recommendations for training: Aqua therapy has been shown in the research to significantly reduce pain, improved physical function, strength, and quality of life (Hinman, Rana S., et al 2007), stretching ITB, hip flexors, quadriceps and hamstrings, strengthening weaker hip abductors(glute medias/minimus). Strengthening specifically hip abductors in various studies when compared to general strengthening resulted in s significant reduction in knee pain, objective change in functional outcome tests, physical function and daily activities (Bennell,K.L., et al. 2010 & Hernández-Molina, G et al. 2008). Core strengthening shoulder also is an integral part of the training program.

Figure 9. Dynamic stabilization Training
c. ACL injury(Anterior cruciate ligament injury)
Recommendations for training: should focus on hamstring strengthening. Strengthening the hamstrings biomechancally transfers the load from the front of the knee to the back, thereby decreasing the stress to the ACL. Neuromuscular training as seen in figure 9, is very effective. It challenges the connection between the nervous and musculoskeletal system requiring the client to stabilize the entire kinematic chain. Research has shown neuromuscular training reduces ACL injuries (HUBSCHER, M. 2010 & Griffin LY, et al., 2006). Core strengthening should be multidirectional in nature as seen in figure 10.

Figure 10. Multidirectional
Training
In the picture on the left, left trunk rotation involves the internal/external obliques, atissimus withdorsi, and right glute medius and minimus muscles to stabilize, as the left glute medius and minimus to stabilize. With the yellow cord applied from the back, this engages the abs primarily to stabilize (from the front) accompanied by the obliques to stabilize, which the low back extensor muscles contract to prevent being pulled backwards. It is important to include dynamic training focusing on hamstrings, glute medius, maximus. Closed chain strengthening (CKC) exercises, such as diagonal forward and diagonal reverse lunges are not only functional, but replicate many common sports as soccer, football and basketball accordingly.
Contrainidications/Precautions: Avoid leg extension exercises completely this causes an anterior translation(shearing) of the tibia on the femur/stressing the graft. Therefore, the exercise is contraindicated. *Biomechanically, shearing stress on the ACL is greatest from 30 degrees of knee flexion to full extension.
Recommendations for training: American Academy of Orthopedic Surgeons (AAOS) Guidelines Post Therapy:
• Continuation of closed kinetic chain exercises(ie. reverse lunges, diagonal lunges,
forward lunge with medicine ball trunk rotation)
• 3 ½ months light jogging begins
• 4 months running begins
• 4 months introduction of plyometrics
• Surgical reconstruction typically sidelines athlete for 6-9 months and once cleared by physician can return to sport activities.
The knee is a dynamic joint that is comprised of a multitude of ligaments, tendons,
connective tissue, muscles that synergistically initiate and correct movement, and
stabilize when an unstable environment. Understanding the anatomy, biomechanics
and weak links of the knee, common injuries and evidenced based training strategies, should provide you with the insight to better understand and work with clients with these kind of injuries more confidently.
Written by Chris Gellert, PT, MMusc & Sportsphysio, MPT, CSCS, AMS.
![]() Chris is the CEO of Pinnacle Training & Consulting Systems (PTCS). A continuing education company, that provides educational material in the forms of home study courses, live seminars, DVDs, webinars, articles and min books teaching in-depth, the foundation science, functional assessments and practical application behind Human Movement, that is evidenced based. Chris is both a dynamic physical therapist with 14 years experience, and a personal trainer with 17 years experience, with advanced training, has created over 10 courses, is an experienced international fitness presenter, writes for various websites and international publications, consults and teaches seminars on human movement. For more information, please visit www.pinnacle-tcs.com.
Chris is the CEO of Pinnacle Training & Consulting Systems (PTCS). A continuing education company, that provides educational material in the forms of home study courses, live seminars, DVDs, webinars, articles and min books teaching in-depth, the foundation science, functional assessments and practical application behind Human Movement, that is evidenced based. Chris is both a dynamic physical therapist with 14 years experience, and a personal trainer with 17 years experience, with advanced training, has created over 10 courses, is an experienced international fitness presenter, writes for various websites and international publications, consults and teaches seminars on human movement. For more information, please visit www.pinnacle-tcs.com.
REFERENCES
Bennell, K.L., et al., 2010, ‘Hip strengthening reduces symptoms but not knee load in people with medial knee osteoarthritis and varus malalignment: a randomized controlled trial,’ Journal of Osteoarthritis and Cartilage, vol. 18, issue 5, pp. 621-628.
Bolgla, L, et al., 2008, ‘Hip Strength and hip and knee kinematics during stair descent in females with and without patellofemoral pain syndrome,’ JOSPT, vol. 38, pp. 12-18.
Cicanowski, H et al., 2007, ‘Hip strength in collegiate female athletes with patellofemoral pain,’ Medicine Science Sports Exercise, vol. 39, pp. 1227-1232.
Frobell, R., et al 2010, ‘A Randomized Trial of Treatment for Acute Anterior Cruciate Ligament Tears,’ New England Journal of Medicine, vol. 363, issue 4, pp. 331-341.
Griffin LY, et al., 2006, ‘Understanding and preventing noncontact anterior cruciate ligament injuries: a review of the Hunt Valley II Meeting, January 2005, American Journal Sports Medicine, vol. 234, pp. 1512-1532.
Hernández-Molina, G., et al., 2008, ‘Effect of therapeutic exercise for hip osteoarthritis pain: Results of a meta-analysis,’ Journal of Arthritis Care & Research, vol. 59, issue 9, pp. 1221–1228.
Hinman, Rana S., et al 2007, ‘ Aquatic Physical Therapy for Hip and Knee Osteoarthritis: Results of a Single-Blind Randomized Controlled Trial,’ Journal of Physical Therapy, vol. 87, no. 1, pp. 32-43.
HU ̈ BSCHER, M., et al., 2010, ‘Neuromuscular Training for Sports Injury Prevention: A Systematic Review,’ American College of Sports Medicine, pp. 413-421.
Khayambashi, H., et al., 2012, ‘The Effects of Isolated Hip Abductor and External Rotator Muscle Strengthening on Pain, Health Status, and Hip Strength in Females With Patellofemoral Pain: A Randomized Controlled Trial, ‘Journal of Orthopedic Physical Therapy, vol. 42, no. 1, pp. 22-29.
Landry SC, et al., 2007, ‘Neuromuscular and lower limb biomechanical differences exist between male and female elite adolescent soccer players during an unanticipated side-cut maneuver,’ American Journal of Sports Medicine, vol. 3, pp. 1888–1900.
Lankhorst, N, et al, 2012, ‘Risk Factors for Patellofemoral Syndrome: A Systematic Review,’ JOSPT, vol. 42, No. 2, pp. 81-90.
Meira, E., et al., 2011, ‘Influence of the Hip on Patients With Patellofemoral Pain Syndrome,’ Sports Health, vol. 3, issue 5, pp. 455–465.
Prins, 2009,’ Females with patellofemoral pain syndrome have weak hip muscles: a systematic review, Australian Journal of Physiotherapy, vol. 55, issue 1, pp. 9-15.
Robinsion, R et al., 2007, ‘Analysis of hip strength in females seeking physical therapy treatment for unilateral patellofemoral pain syndrome,’ JOSPT, vol. 37, pp. 232-238
In the United States more than 700,000 people suffer a stroke each year. Approximately 2/3 of these individuals survive the cerebral vascular accident and require rehabilitation (relearn skills that are lost when part of the brain is damaged). The goals of rehabilitation are to help survivors become as independent as possible and to attain the best possible quality of life.
Physical therapists specialize in treating disabilities related to motor and sensory impairments. They are trained in all aspects of anatomy and physiology related to normal function, with an emphasis on movement. They assess the patient’s strength, endurance, range of motion, gait abnormalities and sensory deficits to design individualized rehabilitation programs aimed at regaining control over motor functions.
Functions compromised when a specific region of the brain is damaged by stroke can sometimes be taken over by other parts of the brain. This ability to adapt and change is known as neuroplasticity. Physical therapists help the patient regain the use of stroke-impaired limbs, teach compensatory strategies to reduce the effect of remaining deficits and establish ongoing exercise programs to help people retain their newly learned skills. The repetitive use of impaired limbs encourages brain plasticity!
In general, physical therapy emphasizes practicing isolated movements, repeatedly changing from one kind of movement to another and rehearsing complex movements that require a great deal of coordination and balance. Balance retraining may consist of walking up or down stairs or moving safely between obstacles. People too weak to bear their own weight can still practice repetitive movements during hydrotherapy (water providing a sensory stimulation and allowing for weight support) or while being partially supported by a harness. A recent trend in physical therapy emphasizes the effectiveness of engaging in goal-directed activities, such as playing games, to promote coordination, balance and movement strategies.
If you or your loved one has had a stroke, be sure to be evaluated by a physical therapist as they can substantially help people achieve the best possible long-term outcome.
Recent research findings have shown that a minority of clients with Parkinson’s do fine without any form of rehabilitation. However, the majority of studies have shown that clients improved in their ability to do daily living activities in response to physical therapy rehabilitation. 62% of research participants who received physical therapy intervention had a successful outcome relative to 38% of the participants in the control group who had a successful outcome. (Murphy & Tickle-Degnen, 2011). In another research project, Tests Predict Falls in Parkinson’sPatients, published in the June 23, 2010 issue of Neurology, looked at 101 Parkinson’s patients who were able to walk without aids. They tested for symptoms such as visual function, balance, gait, strength, reaction time and proprioception. Those who did poorly on the balance tests, mobility tests and coordinating multi-joint movements were more prone to falls (42%).
 People with minor motor system disorders to severe disorders will find that physical therapy can help with the rigidity, slow movement patterns, postural instability, impaired balance and coordination that seem to evolve along with this disease. The physical therapist will evaluate for Functional Gait Testing, Functional Reach Testing, Timed Get Up and Go Test, Bed mobility screening and orthopedic evaluations for mobility and strength.
People with minor motor system disorders to severe disorders will find that physical therapy can help with the rigidity, slow movement patterns, postural instability, impaired balance and coordination that seem to evolve along with this disease. The physical therapist will evaluate for Functional Gait Testing, Functional Reach Testing, Timed Get Up and Go Test, Bed mobility screening and orthopedic evaluations for mobility and strength.
After the evaluation, the physical therapist may set up a specific exercise or movement lesson that uses high amplitude movements that overcome bradykinesia and hypokinesia (activating excessively slow motion).
My personal experience with Parkinson’s patients is one of inquiry, fun and resolution. We even use dance as a means of increasing balance and coordination. When it is a mobility problem like getting out of bed, the physical therapist will create a home program with specific exercises for your needs. When it is a postural instability issue, we will work with balance/gait on different surfaces as well as strengthening for your back, legs, abdomen and torso.
Let the field of physical therapy evaluate and assess what we can do for you!