Parkinson’s Bone Health: Camptocormia
Welcome back fighters, care-partners and fitness professionals! At Bridges For Parkinson’s, posture/vertical stability is a big concern and one we address in every class. Why? Because a strong, vertical spine means reduced falls, better gait, less back pain, increased lung capacity, ability to enjoy activities and live independently. However, fitness professionals observe some folks living with Parkinson’s disease having a severe forward lean at a 45-90 degree angle.
What is this? What causes it? And, is there a solution?
This forward lean is called “Camptocormia”, derived from two Greek words: Kampto- (To bend) and Kormos (trunk). Camptocormia was first documented in the 17th century by the Spanish painter Francisco de Zurbaran. In the 19th century, Brodie wrote about it. Later the term was coined by Rosanoff and Saloff who described the abnormality in World War 1 soldiers traumatized by shell shocks.
Camptocormia is defined as bent spine syndrome (BSS), an abnormal flexion of the trunk, appearing in standing position, increasing during walking and abating in supine position.
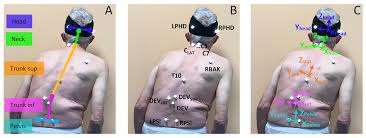
According to Srivanitchapoom and Hallett, approximately 3%-17% of the Parkinson’s population suffers from Camptocormia. See below examples of Camptocormia syndrome.

What Causes “Camptocormia”?
From a muscular perspective, the paraspinal, hip and glute muscles are in a weakened state making it difficult for the body to “fight back” against the neurological side of Camptocormia which we will discuss later in this article.
The paraspinal muscles are located on the left and right side of your spine and are made up of three groups.
- Iliocostalis
- Longissimus
- Spinalis
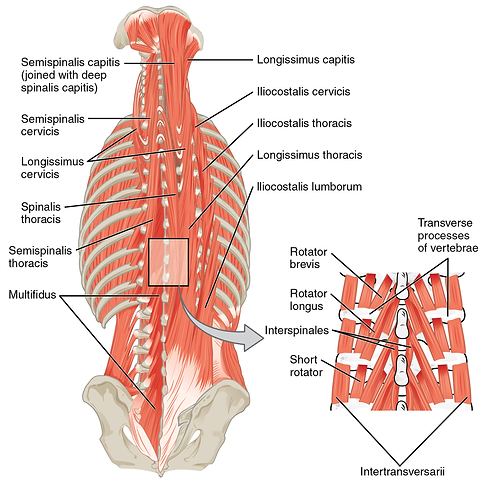
Paraspinal muscles
The job of the paraspinal muscles is to extend your spine and to bend it over to the same side on which the contracting paraspinal muscle is located. For example: bending to the side to pick something off the floor.
The four main hip and glute muscles include:
- The gluteal group (butt muscles) – responsible for stabilizing the upper body and pelvis, aid in locomotion and extend the hip. Example: when your leg travels behind you before kicking a ball.
- The adductor group – responsible for pulling the thighs together and rotating the upper leg inward and stabilizing the hip. Example: When the leg moves to the center of the body after stepping out for a half-jumping jack..
- The lateral rotator group – responsible for rotating the hip joint laterally. Additionally this group will aid in extension and adduction of the hip. Example: Piriformis stretch also known as the “figure 4 stretch”
- The iliopsoas – this is the primary hip flexor and assists with external rotation of the hip joint. It plays an important role in correct posture for standing/sitting lumbar position and walking/running.
These muscle groups play a vital part in your activities of daily living! Bridges For Parkinson’s addresses these muscles groups with exercises such as:
- Sit to stands
- Squats
- Bridges/Bird dog/Seated Back Extension (with tubes)
- Clamshells
- ½ Warrior step
- Deadlifts
- Lunges (forward, reverse, lateral and diagonally)
- Rows
- T’s
And we progress the exercise to a higher level of difficulty by:
- Standing on one leg
- Adding repetitions or length of time
- Standing on the BOSU/Pad
Now, let’s discuss the neurological aspect of Camptocormia. Much like “Pisa Syndrome”, the root cause is multifactorial and largely unknown.
Camptocormia is largely considered a neurological disorder due to its comorbidity with other neurodegenerative and movement disorders such as ALS, dementia with Lewy Bodies, Alzheimer’s, and Parkinson’s (Srivanitchapoom & Hallett, 2016). As mentioned, although the presentation of this disorder is largely based on the forward lean, with a tendency to worsen throughout the day due to muscle fatigue, the causes are up for debate in research. For now, the best guess we can take is that the association with PD and other dystonias translates to a faulty cascade of events in the major movement centers of the brain, and the brain-body connection as consequence (Margraf et al., 2016).
Typically, you will find Camptocormia in the more advanced stages of PD, such as those living with Parkinson’s for 7 or more years, those with previous spinal issues, and those who indicate lower motor function on neurological exams (Srivanitchapoom & Hallett, 2016). However, even if you meet any/all of these criteria you won’t necessarily develop this disorder.
The onset of Camptocormia can be mitigated with proper preventative care such as exercise and physical/occupational therapy. Additionally, for individuals with this syndrome, botox and surgery (DBS) can alleviate the severe forward lean.
Botox may be used as a treatment that “freezes” the muscles affected in this disorder, allowing the muscles to lengthen, in turn helping to improve posture. However, this is neither a permanent nor strong solution, although it is seemingly effective in smaller studies assessing the benefits of this treatment (Bertram et al., 2015; Todo et al., 2018; Anandan et al., 2021) . There are also long term drawbacks, the biggest one being muscle weakness that can cause overall worsening of the disorder. There are other, more permanent ways of managing this as well, but are much more invasive. Spinal surgery and Deep Brain Stimulation are two of the more “common” options, although to be considered for these the symptoms must be severe (Margraf et al., 2016). The best ways to manage this disorder are to continue taking your prescribed medication, and exercise to strengthen the muscles involved with keeping your posture upright.
How Does Camptocormia Affect Activities of Daily Living?
Similar to Pisa syndrome, Camptocormia is a non-fixed flexion of the trunk, which can lead to significant deficits in posture, balance, safety, and ability to perform daily activities. Posture is one of the pivotal components for ALL ADLs. So, from an occupational therapy scope, restoration of posture and maintenance of current occupational performance is key.
ADL training: due to posture changes when standing, patients may experience difficulty maintaining routine activities with dressing, bathing. ADL retraining helps to maintain independence and current level of occupational performance.
Seating and positioning: in order to promote improved posture, position hips in an anterior angle, which can allow for increased participation in ADL’s such as feeding or grooming. This can also help with visual ability and increase social participation. Positioning during sleep is another potential area to examine as we do not want to encourage further postural deformity.
Visual strategies: due to the posture changes while standing, camptocormia can lead to difficulty interacting with our environment as we typically would, especially visually. Implementing visual cues or compensatory strategies can help promote improved posture and allow for safe interaction within their home or social environment.
Examples of Cues
1. Sit/stand with shoulders down and shoulder blades pinched together as if you are royalty. Automatically, people position their head over the shoulders and sit/stand taller.
2. Walk with eyes lifted and looking in the distance. When people look down they tend to bend over and slump their shoulders. Looking in the distance prepares them for what is ahead and trains them to use peripheral vision for what is right in front of them.
Home Modifications: modifying home and using assistive devices such as installing grab bars, removing trip hazards (rugs), training with reacher will ensure safety and promote ADL participation.
Energy conservation: as the day continues and the patient feels more fatigued, posture will be more difficult to maintain. Learning and implementing energy conservation techniques could help to promote improved posture throughout the day.
Supine exercises: Supine exercises (on your back) will help to maintain muscle strength and endurance while maintaining proper posture throughout range of motion. These exercises eliminate gravitational pull and forward flexion due to Camptocormia.
In closing, Camptocormia is unique in that it develops over time in conjunction with a movement disorder. The strength of your physical structure depends on having the knowledge to identify possible bone issues such as Camptocormia, properly addressing the issue with corrective exercises and a team that provides support and encouragement.
Bridges For Parkinson’s focuses on helping our fighters and care-partners develop a sense of awareness, provide corrective exercise therapy for those dealing with Camptocormia or preventative exercises to support a strong, vertical spine!
Fit Pros: You Can Improve the Lives of Those Living with Parkinson’s
Enroll in Colleen’s 12-hour online course, Parkinson’s Disease Fitness Specialist. The course brings the research, medical and fitness fields together so that fitness professionals gain a comprehensive understanding of Parkinson’s disease, and learn how to work with those who have it.

Originally printed on bridgesforparkinsons.com. Reprinted with permission.
Written by:
- Colleen Bridges, M.Ed., NSCA-CPT, Parkinson’s Disease Fitness Specialist
- Renee Rouleau, PhD candidate, Jacobs School of Biomedical Sciences, University at Buffalo
- Betsy Lerner, ISSA-CPT, MA English and African American Lit, Parkinson’s Disease Specialist and Rock Steady Boxing Certified
- Cindy Nyquist, LPTA, ATC, Rock Steady Boxing Certified
References
- Anandan, C., & Jankovic, J. (2021). Botulinum Toxin in Movement Disorders: An Update. Toxins, 13(1), 42. MDPI AG. Retrieved from http://dx.doi.org/10.3390/toxins13010042
- Djaldetti R, Mosberg-Galili R, Sroka H, et al. Camptocormia (bent spine) in patients with Parkinson’s disease-characterization and possible pathogenesis of an unusual phenomenon. Mov Disord. 1999;14:443–7.
- Margraf NG, Wrede A, Deuschl G, Schulz-Schaeffer WJ. Pathophysiological Concepts and Treatment of Camptocormia. J Parkinsons Dis. 2016 Jun 16;6(3):485-501. doi: 10.3233/JPD-160836. PMID: 27314757; PMCID: PMC5008234.
- Schäbitz WR, Glatz K, Schuhan C, et al. Severe forward flexion of the trunk in Parkinson’s disease: focal myopathy of the paraspinal muscles mimickingcamptocormia. Mov Disord. 2003;18:408–14.
- Srivanitchapoom P, Hallett M. Camptocormia in Parkinson’s disease: definition, epidemiology, pathogenesis and treatment modalities. J Neurol Neurosurg Psychiatry. 2016 Jan;87(1):75-85. doi: 10.1136/jnnp-2014-310049. Epub 2015 Apr 20. PMID: 25896683; PMCID: PMC5582594.
- Todo, H., Yamasaki, H., Ogawa, G. et al. Injection of Onabotulinum Toxin A into the Bilateral External Oblique Muscle Attenuated Camptocormia: A Prospective Open-Label Study in Six Patients with Parkinson’s Disease. Neurol Ther 7, 365–371 (2018). https://doi.org/10.1007/s40120-018-0108-x
- Wartenberg R. Camptocormia. Arch Neurol Psychiatry. 1946;56:327.