Do You Slouch? Improve Your Health with Better Posture
When babies learn to sit, they elongate their spine, which is naturally efficient and comfortable. Moreover, it provides the most skeletal support without requiring a lot of muscle strength. Despite this, around 4-years old, most of us began to slump. Why? Well, significantly, it’s probably because we started school and began spending more time sitting.
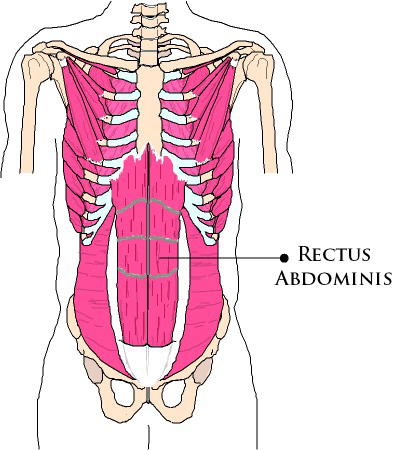
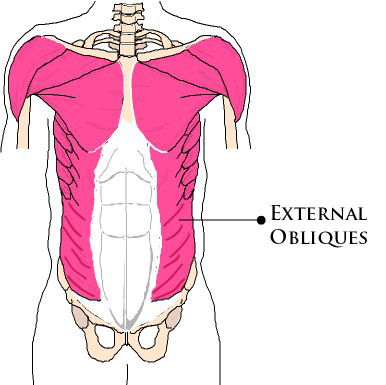
Poor posture often results from weak core muscles, and weak core muscles contribute to slouching. Also, most neck pain not caused by trauma is usually the result of poor posture and weak muscles supporting our head. For example, sitting at our computers, or hunching over our phone for several hours can strain our neck, and shoulders.
More importantly, strong core muscles lessen wear and tear on the spine. And that prevents falls and injuries. Strengthening your abdominal muscles improves your posture and enhances balance and stability.
You might not notice these actions: putting on shoes, picking up a package, or turning to look behind you, until they become difficult or painful. Core-centric activities include acts that spring from, or pass through, the core: lifting, twisting, carrying, hammering, reaching overhead — even vacuuming, mopping, and dusting.
What is Good Posture?
Good posture doesn’t mean standing like a stiff piece of board. Many people overcompensate for bad posture by standing up too straight. When our posture is correct, our ears, shoulders, hips, knees, and ankles align naturally. Good posture looks natural and relaxed.
Don’t Slouch! There is Power in Good Posture
Maintaining good posture is not easy. And despite the importance of good posture, most of us don’t do anything to improve it. As a result, we go about our lives uncomfortably hunching our backs and slouching. Practicing good posture strengthens our abdominal muscles and builds low back stability. If these muscles are weak, we’re more apt to slouch. For example, we may start the day sitting upright, but soon we’re lost in our work and slouching once again.
Good posture has many benefits. It aligns your body, and makes you look taller (you can lose 2 inches by slouching). Good posture even speeds up your metabolism (burn up to 350 calories a day). At the same time, having good posture reduces pain by using your muscles to support your skeleton) and improves your mood. (Don’tSlouch)
How to Improve Your Posture
Proper posture includes alignment, balance, and alignment. You’ll see immediate improvements in your posture by practicing the following two exercises. All you need is a wall. These two, quick and easy exercises realign and strengthen your muscles and ease pain and achiness that results from poor posture.

Exercise 1: The Chin Tuck is an exercise to strengthen your neck muscles. Start standing with your back to a wall. Extend your neck, keeping your gaze forward, and lean back so the back of your head touches the wall. You can also place a pillow behind your head if you can’t move all the way back. Keep your gaze forward, so that your chin is parallel with the floor. Retract your chin towards the wall until you you’re your neck muscles contract, then release the contraction. Repeat this movement 10 times.

Exercise 2: Wall Angels stretch your chest muscles, improve shoulder range of motion, and strengthen your upper back. Start standing with your back and head against a wall and your feet about 6 inches from the wall. With your arms at your side, face your palms forward. Slide your arms out to the side along the wall, bending your elbows at a 90-degree angle. Continue sliding your arms up along the wall to about 45 degrees above your shoulder. Stop when you feel your shoulders elevate or if you feel pain. Return your arms back down to the starting position. Repeat 10 times.
Jacqueline Gikow, is the owner of Audacious Living NYC™. Her holistic, health and wellness practice centers on pain relief through better movement. She is certified through the National Association of Sports Medicine (NASM), the National Board of Medical Examiners (NBCHWC), the Functional Aging Institute (FAI), Medfit (MFN), and the Arthritis Foundation (AFAP/AFEP). Her fitness practice includes in-home and remote, one-on-one fitness training and coaching in New York City. Jacqueline Gikow can be reached at: https://audaciouslivingnyc.com, or on Facebook: https://www.facebook.com/groups/audaciouslivingnyc
References
https://www.madisondias.com/posture/dont-slouch-the-power-of-good-posture/
http://lifehacker.com/fix-your-posture-with-these-three-simple-exercises-1754621367