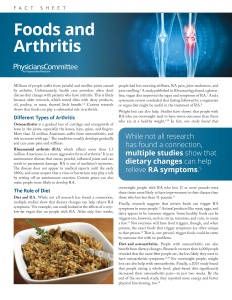
Food and Arthritis
Millions of people suffer from painful and swollen joints caused by arthritis. Unfortunately, health care providers often don’t discuss diet change with patients who have arthritis. This is likely because older research, which tested diets with dairy products, oil, poultry, or meat, showed little benefit. Current research shows that foods can play a substantial role in arthritis.
Different Types of Arthritis
Osteoarthritis is a gradual loss of cartilage and overgrowth of bone in the joints, especially the knees, hips, spine, and fingers. More than 32 million Americans suffer from osteoarthritis, and risk increases with age. The condition usually develops gradually and can cause pain and stiffness.
Rheumatoid arthritis (RA), which affects more than 1.3 million Americans, is a more aggressive form of arthritis. It is an autoimmune disease that causes painful, inflamed joints and can result in permanent damage. RA is one of medicine’s mysteries. The disease does not appear in medical reports until the early 1800s, and some suspect that a virus or bacterium may play a role by setting off an autoimmune reaction. Certain genes can also make people more likely to develop RA.
The Role of Diet
Diet and RA. While not all research has found a connection, multiple studies show that dietary changes can help relieve RA symptoms. For example, one study looked at the effects of a very-low-fat vegan diet on people with RA. After only four weeks, people had less morning stiffness, RA pain, joint tenderness, and joint swelling. A study published in Rheumatology found a gluten-free, vegan diet improved the signs and symptoms of RA. And a systematic review concluded that fasting followed by a vegetarian or vegan diet might be useful in the treatment of RA.
Download the Physicians Committee for Responsible Medicine’s Fact Sheet, Food and Arthritis, to read the rest of this article. Feel free to download and share this free resource.
The Physicians Committee for Responsible Medicine is a 501(c)(3) nonprofit organization, headquartered in Washington, DC. Our efforts are dramatically changing the way doctors treat chronic diseases such as diabetes, heart disease, obesity, and cancer. By putting prevention over pills, doctors are empowering their patients to take control of their own health.
Fact sheet shared with permission from PCRM. Click here to view other PCRM Fact Sheets.