Aquatic Rehabilitation Post Joint Replacement
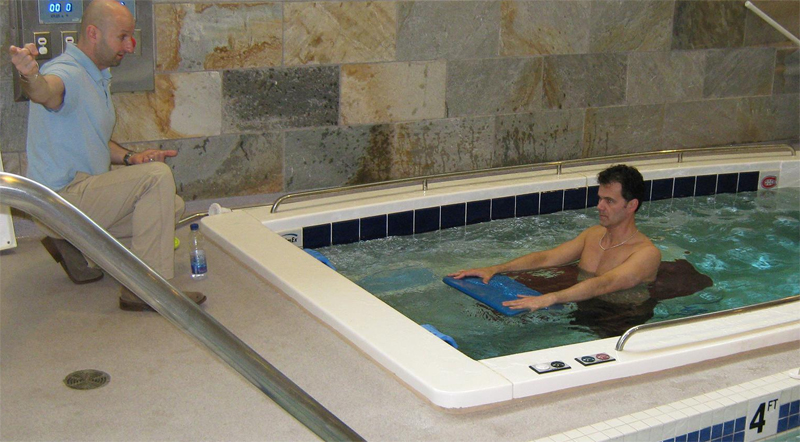
The most common symptoms a client experiences after undergoing a total joint replacement are pain, swelling, stiffness, muscle weakness and limited activities of daily living. Traditional rehabilitation for patients following a total joint replacement typically involves some combination of range of motion, strengthening…




 You just found out you are pregnant! Congratulations!
You just found out you are pregnant! Congratulations! 2. Mountain Pose: (pictured right) A body in alignment moves and functions more efficiently. Try taking a deep breath while you slump in a chair. Difficult, right? In pregnancy, many women surrender to gravity and its disproportionate effect on physical alignment. Practice Mountain Pose often throughout your day to familiarize your nervous system with this posture. Over time, your posture will improve.
2. Mountain Pose: (pictured right) A body in alignment moves and functions more efficiently. Try taking a deep breath while you slump in a chair. Difficult, right? In pregnancy, many women surrender to gravity and its disproportionate effect on physical alignment. Practice Mountain Pose often throughout your day to familiarize your nervous system with this posture. Over time, your posture will improve. 3. Squat: (pictured right) Could there be a more perfect exercise to do during pregnancy? Let’s count the benefits.
3. Squat: (pictured right) Could there be a more perfect exercise to do during pregnancy? Let’s count the benefits.


