Are you being carried away the tide?
 Are you being carried away the tide?
Are you being carried away the tide?
The best analogy I’ve come up with while working with clients to describe how most people live their lives is that they get carried away by the tide.
Imagine the powerful ocean currents pulling you in whichever direction they wish.
Life can have the same effect. People, circumstances, and indecision can carry anyone away into the tide if you let it.
It’s how people lose track of their priorities and find themselves unhealthy.
I believe this is why people are unhappy in jobs, relationships, and with life in general. Because we think life is out of our control. We forget that we get to choose.
So, if you catch yourself thinking that a situation you’re unhappy with just “is what it is,” that’s a sign you’re being carried away in the tide.
We can change any circumstance in our lives, even if it’s just changing how we perceive it. If that’s something you’d like support with regarding your health, I’d love to chat.
In conclusion, the next time someone asks you if you are being carried away by the tide, you can say: “Not anymore!”
Originally printed on Move Well Fitness blog. Reprinted with permission.
Maurice D. Williams is a personal trainer and owner of Move Well Fitness in Bethesda, MD. With almost two decades in the industry, he’s worked with a wide range of clients, including those with health challenges like diabetes, osteoporosis, multiple sclerosis, hypertension, coronary artery disease, lower back pain, pulmonary issues, and pregnancy. Maurice is also a fitness educator with Move Well Fit Academy and NASM.
 Probiotics:
Probiotics:
 We all have moments like the one I am describing here in our lives that catch our attention. It is important to know that when we DO experience loss or change on a large scale that we become “active participants” in responding to the circumstances that are presented to us. We need to take action – positive action – in order to alter the course of our lives. It is through adjusting to the changes and challenges of life as we grow into maturity (and hopefully wisdom) that we can appreciate what we have been given.
We all have moments like the one I am describing here in our lives that catch our attention. It is important to know that when we DO experience loss or change on a large scale that we become “active participants” in responding to the circumstances that are presented to us. We need to take action – positive action – in order to alter the course of our lives. It is through adjusting to the changes and challenges of life as we grow into maturity (and hopefully wisdom) that we can appreciate what we have been given. RUNNING: I have been a runner since 1964 and have accumulated over 65,000 miles over that span. It is the foundation from which I “grew older and not old”. It is as close to my heart as breathing itself and I am now focusing on increasing my speed while running between 5 and 7 miles 3 days a week. I am now able to average under 6:00 per mile pace for the distances I use and am doing so on a treadmill to save wear and tear going forward. Cycling has helped my running immensely and my legs are stronger as a result.
RUNNING: I have been a runner since 1964 and have accumulated over 65,000 miles over that span. It is the foundation from which I “grew older and not old”. It is as close to my heart as breathing itself and I am now focusing on increasing my speed while running between 5 and 7 miles 3 days a week. I am now able to average under 6:00 per mile pace for the distances I use and am doing so on a treadmill to save wear and tear going forward. Cycling has helped my running immensely and my legs are stronger as a result.

 minutes a week of moderate-intensity aerobic physical activity. They also suggest muscle-strengthening activities that are moderate or high intensity and involve all major muscle groups on 2 or more days a week. As baby boomers, we can have a pretty busy schedule. As a 50 something baby boomer myself, I juggle quite a bit of activities in a day. I’m not complaining though, life at this stage of the game is exciting. It’s refreshing to see older adults doing more than ever before. Ironically, the busier our lifestyles are, the more we need the benefits of exercise but find that time becomes harder to come by.
minutes a week of moderate-intensity aerobic physical activity. They also suggest muscle-strengthening activities that are moderate or high intensity and involve all major muscle groups on 2 or more days a week. As baby boomers, we can have a pretty busy schedule. As a 50 something baby boomer myself, I juggle quite a bit of activities in a day. I’m not complaining though, life at this stage of the game is exciting. It’s refreshing to see older adults doing more than ever before. Ironically, the busier our lifestyles are, the more we need the benefits of exercise but find that time becomes harder to come by. Beginner Total Body Circuit:
Beginner Total Body Circuit:
 “Just relax.”
“Just relax.” Breathe
Breathe Athletes have many questions about energy bars:
Athletes have many questions about energy bars: Gluten-free: Bonk Breaker, BumbleBar, Elev8Me, Enjoy Life, Enjoy Life, EnviroKidz Rice Cereal, Fody, Good Belly, GoMacro, Hammer, KIND, Lara, Picky, PowerBar Protein Plus, Pure Protein, ProBar, RX, Quest, Raw Revolution, That’s It Fruit, thinkThin, Truwomen, Zing, 88 Acres Seed and Oat.
Gluten-free: Bonk Breaker, BumbleBar, Elev8Me, Enjoy Life, Enjoy Life, EnviroKidz Rice Cereal, Fody, Good Belly, GoMacro, Hammer, KIND, Lara, Picky, PowerBar Protein Plus, Pure Protein, ProBar, RX, Quest, Raw Revolution, That’s It Fruit, thinkThin, Truwomen, Zing, 88 Acres Seed and Oat.
 But what if you trade your expectations for appreciation? Appreciate the fact that you are able to exercise, that you have a wonderful family or great friends, or that you’re resourceful enough to eventually reach your outcome.
But what if you trade your expectations for appreciation? Appreciate the fact that you are able to exercise, that you have a wonderful family or great friends, or that you’re resourceful enough to eventually reach your outcome.
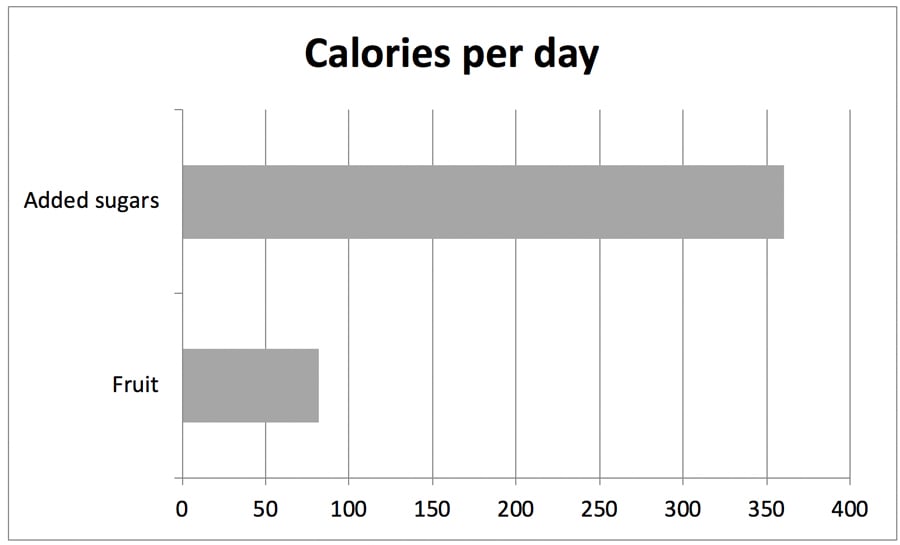
 Sure, there’s nothing new about saying added sugar is bad for you (regardless of your age). Your mom told you, and your doctor says so, too, but you can’t sugar-coat the truth — you love the sweet stuff. So what else is new? Well, it turns out that there is something that is both new and troubling about sugar.
Sure, there’s nothing new about saying added sugar is bad for you (regardless of your age). Your mom told you, and your doctor says so, too, but you can’t sugar-coat the truth — you love the sweet stuff. So what else is new? Well, it turns out that there is something that is both new and troubling about sugar.